OVERVIEW
• Iron deficiency is the commonest cause of anaemia worldwide
• Iron deficiency is usually easily diagnosed from the red cell indices
• A drop in haemoglobin is generally a late feature of iron deficiency
• The serum ferritin is a reliable means of confirming the diagnosis but may be falsely normal or even elevated as a reactive phenomenon as ferritin is an acute phase protein
• Iron deficiency is not a diagnosis in itself and in males and postmenopasual women blood loss from the gastrointestinal tract must be excluded
• Oral iron is preferred for iron replacement therapy, but occasionally parenteral iron is required
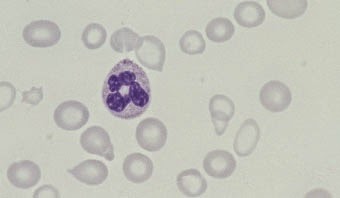
Iron deficiency is the commonest cause of anaemia worldwide and is frequently seen in general practice. Iron deficiency anaemia is caused by defective synthesis of haemoglobin, resulting in red cells that are smaller than normal (microcytic) and contain reduced amounts of haemoglobin (hypochromic).
Iron metabolism
Iron has a pivotal role in many metabolic processes, and the average adult contains 3–5 g of iron, of which two-thirds is in the oxygen- carrying molecule haemoglobin.
A normal Western diet provides about 15 mg of iron daily, of which 5–10% is absorbed (~ 1 mg), principally in the duodenum and upper jejunum, where the acidic conditions help the absorption of iron in the ferrous form. Absorption is helped by the presence of other re- ducing substances, such as hydrochloric acid and ascorbic acid. The body has the capacity to increase its iron absorption in the face of in- creased demand, for example, in pregnancy, lactation, growth spurts and iron deficiency (Box 1.1).
Once absorbed from the bowel, iron is transported across the mucosal cell to the blood, where it is carried by the protein transferrin to developing red cells in the bone marrow. Iron stores comprise fer- ritin, a labile and readily accessible source of iron and haemosiderin, an insoluble form found predominantly in macrophages.
About 1 mg of iron a day is shed from the body in urine, faeces, sweat